
Blog - 17 May 2015: World Hypertension Day
Better access to quality care to stem rising blood pressures in Africa
- May 17, 2015
PharmAccess mobilizes public and private resources for the benefit of doctors and patients through clinical standards and quality improvements, loans for healthcare providers, health insurance, mHealth innovations and operational research.
Better access to quality care to stem rising blood pressures in Africa
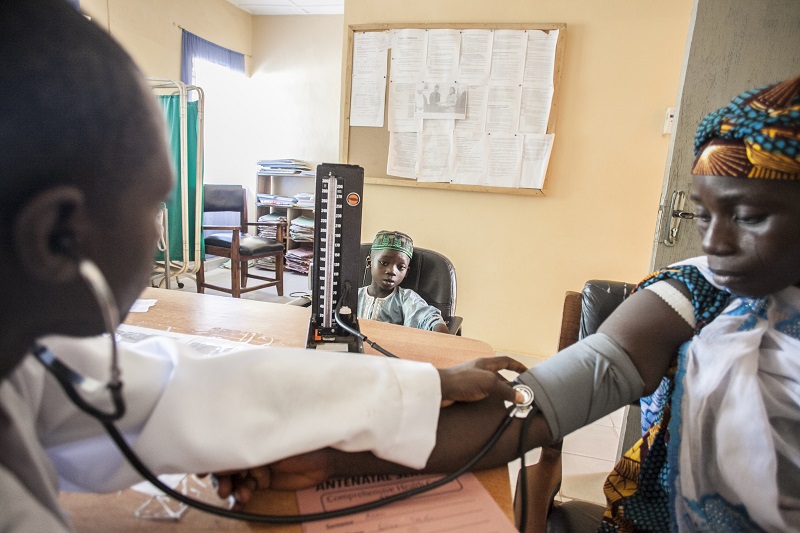
High blood pressure has overtaken childhood underweight as the leading risk factor for death in sub-Saharan Africa (SSA). While the world has been fighting HIV/Aids, malaria, and tuberculosis with millions of dollars, non-communicable, chronic diseases have very rapidly become a serious health problem. Almost half of the adults over 25 years have hypertension in SSA (WHO).
Hypertension can be treated effectively, greatly reducing the risk of cardiovascular diseases. The quality care needed for this can only be implemented in a well-functioning health system. Doctors and nurses need to be trained in the right guidelines, laboratories are needed for diagnostic tests, pharmacies need to have continuous stocks of essential medicine, and systems need to be in place to monitor patients over their lifetime.
However, health systems in most countries in SSA are overburdened. Health facilities struggle with regular drug stock outs, high turnover of doctors, lack of diagnostic tests and non-functioning referral systems.
Consistent healthcare financing is needed to provide patients with better quality of care and long-term access to care. Effective innovations to strengthen weak health systems are needed urgently. A well-functioning health system is a prerequisite for implementing chronic care for people with hypertension, and to combat the rise of cardiovascular diseases in SSA. Left untreated, hypertension can lead to complications that cause early death or disable people, such as stroke. Families lose their breadwinners and are pushed into poverty, while treatment could have prevented this.
Reaching the people most at risk
Emmanuel Sunday*, a Nigerian farmer in his 50s, who lives with his wife and five children in a small rural village in Kwara State, Bacita, has high blood pressure. The hypertension puts him at serious risk to develop a stroke or heart attack, which would be disastrous for him and his family since Sunday is the family’s breadwinner.
With treatment, his chances of getting such a catastrophic disease would substantially reduce. There is one problem: costs of blood pressure treatment are over USD 100 per year. Sunday only earns USD 200 per year and he needs to support his family. So this care is obviously unaffordable for him.
Sunday would greatly benefit from getting health insurance, but that did not exist in his state. In 2007 however, the Kwara State Health Insurance program (KSHI) was introduced, a health insurance program for people on low incomes like Sunday. The program is a public-private partnership of Hygeia Community Health Care, Kwara State government, the Health Insurance Fund, andPharmAccess.
People can enroll into the insurance by paying USD 4 per year, which is 12% of the total premium. The remaining 88% is subsidized by the local government and a decreasing amount of donor money. With their insurance, people can access care in the healthcare clinics that are contracted by the insurer.
Improving quality of care
Access to care alone is not enough, because most clinics in Nigeria are of very poor quality. If there is no doctor and there are no drugs, being insured does not make a difference for people’s health. Therefore, the KSHI program also works on improving the quality of participating clinics. Examples of quality improvement include training of doctors in guideline-based care, upgrading of facilities and equipment and management and administration support.
Research into the program’s impact showed significant health benefits for people with hypertension who enrolled in the program. Their health improved because of the access to better quality of care, i.e. getting diagnosed, receiving the right treatment and ongoing monitoring. Blood pressure fell significantly more in the communities with health insurance compared to communities without health insurance.
The systolic blood pressure reduction that could be attributed to the insurance program was 5 mmHg. This is an important reduction as each 10 mmHg reduction in systolic blood pressure is estimated to reduce the risk of stroke by 38% and the risk of ischemic heart disease by 26%.
Better health systems need smarter financing
The KSHI shows that high-quality cardiovascular disease prevention care can be provided in rural areas in SSA. It did so through influencing both the demand and the supply side. On the demand side, the insurance removed the barrier to seek care as policyholders no longer faced high out-of-pocket expenditures to pay for health services. This enabled them to not just to get diagnosed, but also to get the drugs they need and come back for follow-up check-ups.
On the supply side the quality improvement program included guidelines for hypertension care which were implemented in the program clinics. Quality of care was measured according to international quality standards.
The Kwara State Health Insurance program has proven to make a difference for mister Sunday and many others with hypertension.
* Not his real name